OVERVIEW
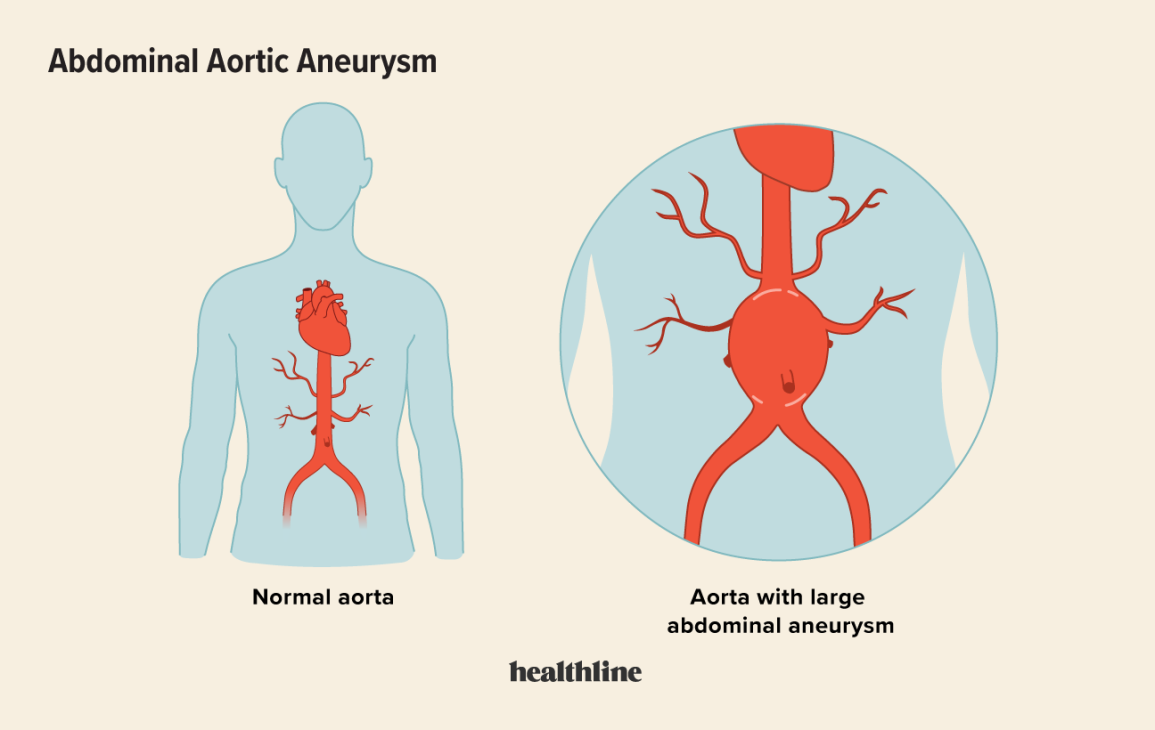
AN ABDOMINAL AORTIC ANEURYSM (AAA) IS A BULGE OR SWELLING IN THE AORTA, THE MAIN BLOOD VESSEL THAT RUNS FROM THE HEART DOWN THROUGH THE CHEST AND TUMMY.
An AAA can be dangerous if it is not spotted early on. It can get bigger over time and could burst (rupture), causing life-threatening bleeding. Screening for AAA is routinely offered by the NHS to all men aged 65 and over. Women aged 70 or over, who have underlying risk factors such as high blood pressure, may also be advised to attend screening for AAA. AAAs do not usually cause any obvious symptoms, and are often only picked up during screening or tests carried out for another reason. Some people with an AAA have:
- a pulsing sensation in the tummy (like a heartbeat)
- tummy pain that does not go away
- lower back pain that does not go away.
If an AAA bursts, it can cause:
- sudden, severe pain in the tummy or lower back
- dizziness
- sweaty, pale and clammy skin
- a fast heartbeat
- shortness of breath
- fainting or passing out
Call 999 for an ambulance immediately if you or someone else develops symptoms of a burst AAA.
WHEN TO GET MEDICAL HELP
Make an appointment to see a GP as soon as possible if you have symptoms, especially if you’re at a higher risk of an AAA.
An ultrasound scan of your tummy may be done to check if you have one.
Call 999 for an ambulance immediately if you or someone else develops symptoms of a burst AAA.
An AAA can form if the sides of the aorta weaken and balloon outwards. It’s not always clear why this happens, but there are things that increase the risk. People at a higher risk of getting an AAA include all men aged 66 or over and women aged 70 or over who have one or more of the following risk factors:
- high blood pressure
- chronic obstructive pulmonary disease
- high blood cholesterol
- a family history of AAA
- cardiovascular disease, such as heart disease or a history of stroke
- they smoke or have previously smoked
Speak to a GP if you’re worried you may be at risk of an AAA. They may suggest having a scan and making healthy lifestyle changes to reduce your risk of an AAA.
The recommended treatment for an AAA depends on how big it is.
Treatment is not always needed straight away if the risk of an AAA bursting is low.
Treatment for a:
- small AAA (3cm to 4.4cm across) – ultrasound scans are recommended every year to check if it’s getting bigger; you’ll be advised about healthy lifestyle changes to help stop it growing
- medium AAA (4.5cm to 5.4cm) – ultrasound scans are recommended every 3 months to check if it’s getting bigger; you’ll also be advised about healthy lifestyle changes
- large AAA (5.5cm or more) – surgery to stop it getting bigger or bursting is usually recommended
Ask your doctor if you’re not sure what size your AAA is.
There are several things you can do to reduce your chances of getting an AAA or help stop one getting bigger.
These include:
- stopping smoking – read stop smoking advice and find out about Smokefree, the NHS stop smoking service
- eating healthily – eat a balanced diet and cut down on fatty food
- exercising regularly – aim to do at least 150 minutes of exercise a week; read about how to get started with some common activities
- maintaining a healthy weight – use the healthy weight calculator to see if you need to lose weight, and find out how to lose weight safely
- cutting down on alcohol – read tips on cutting down and general advice about alcohol
If you have a condition that increases your risk of an AAA, such as high blood pressure, your GP may also recommend taking tablets to treat this.
SCREENING FOR AAAS
In England, screening for AAAs is offered to men during the year they turn 65. This can help spot a swelling in the aorta early on, when it can be treated.
The test involves a quick and painless ultrasound scan to see how big your aorta is.
If you’re a man over 65 and you have not been screened, you can ask for a test by contacting your local AAA screening service directly.
Women aged 70 or other with underlying risk factors such as high blood pressure or chronic obstructive pulmonary disease may also benefit from an ultrasound scan. You will need to ask a GP for a referral as women are not currently routinely invited for scanning.

TREATMENT
THE TREATMENT FOR AN ABDOMINAL AORTIC ANEURYSM (AAA) MOSTLY DEPENDS ON HOW BIG IT IS.
AAAs are grouped into three sizes:
- small AAA – 3cm to 4.4cm across
- medium AAA – 4.5cm to 5.4cm across
- large AAA – 5.5cm or more across
Large AAAs are more likely to burst (rupture), so surgery to stop this happening is usually recommended.
The risk of a small or medium AAA bursting is much lower, so you’ll normally be advised to have regular scans to check its size and make healthy lifestyle changes to help stop it getting bigger.
Ask your doctor if you’re not sure what size your aneurysm is.
SMALL AND MEDIUM AAAS
You might not need treatment if you have a small or medium AAA. This is because the risk of the AAA bursting is smaller than the risk of complications from surgery. You’ll be asked to come back for regular ultrasound scans to check if your aneurysm is getting bigger.
You’ll be asked to come back for regular ultrasound scans to check if your aneurysm is getting bigger.
Scans are done:
- every year if you have a small AAA
- every three months if you have a medium AAA
Surgery may be offered if your aneurysm becomes a large AAA.
You’ll also be told about lifestyle changes that can help reduce the risk of an aneurysm getting bigger, such as eating healthily.
Read more about how to stop an aneurysm growing. You can otherwise carry on as normal, although having an AAA may have some implications for things such as driving and getting travel insurance.
LARGE AAAS
If you have a large AAA, surgery to strengthen it with a piece of man-made tubing (a graft) is usually recommended because the risk of it bursting is bigger than the risk of complications from surgery.
There are two main types of surgery for an AAA:
- endovascular surgery – the graft is inserted into a blood vessel in your groin and then carefully passed up into the aorta
- open surgery – the graft is placed in the aorta through a cut in your tummy
Both techniques are equally good at reducing the risk of an AAA bursting, but each has its own advantages and disadvantages. Talk to your surgeon about which is best for you.
If surgery isn’t suitable for you, you’ll have regular scans to monitor your aneurysm and be given advice about healthy lifestyle changes, and you may be prescribed medication to help stop the aneurysm bursting.
ENDOVASCULAR SURGERY
In endovascular surgery, a graft is inserted into a blood vessel in your groin through small cuts made in your skin. It’s then carefully guided up into the aneurysm. This is usually done under general anaesthetic, where you’re asleep.
You’ll normally stay in hospital for two or three days after the operation, and it’ll take a few weeks or months to fully recover.
The risk of complications is generally lower than with open surgery, and the hospital stay and recovery time is often shorter. Around 98% of people make a full recovery.
Risks of endovascular surgery include:
- the graft leaking or slipping out of position – you’ll have regular scans to check for this, and may need another operation to fix any problems
- a wound infection or infection of the graft
- heavy bleeding from your groin
- a blood clot, heart attack or stroke
OPEN SURGERY
During open surgery, a cut is made in your tummy and your surgeon replaces the affected section of aorta with a graft. This is done under general anaesthetic.
You’ll usually stay in hospital for 7-10 days after the operation, and it’ll take a few weeks or months to fully recover.
The risk of complications is generally higher than with endovascular surgery, and the hospital stay and recovery time is often longer. Around 95-97% of people make a full recovery.
Risks of open surgery include:
- a wound infection or infection of the graft
- a blood clot
- heavy bleeding from your groin
- a heart attack or stroke
- erectile dysfunction or ejaculation problems in men
The risk of graft problems is lower than with endovascular surgery. The graft will usually work well for the rest of your life and you won’t normally need regular scans to check it.
TREATMENT FOR A BURST AAA
A burst aneurysm is treated with emergency surgery using the same techniques used for a large aneurysm.
The decision about whether to perform open or endovascular surgery is made by the surgeon carrying out the operation.
Only about 2 in 10 people who have a burst aneurysm survive, which is why an operation to stop an aneurysm bursting is usually recommended if it’s large.